
COVID-19 herd immunity in Stockholm County
Published September 17th, 2020 under Editorial
The point of this post is to encourage people to look at COVID-19 herd immunity in a more analytical way. It worries me when I see so many people reacting to things based on emotion rather than analysis.
There has been a lot of chatter online regarding herd immunity since the beginning of the COVID-19 pandemic. I often see people referring to Sweden as a failed experiment in herd immunity, but I do not understand why.
Why Stockholm County?
Sweden as a whole is one of the few countries which did not enforce a strict lockdown for COVID-19. Their advice over time has been fairly consistent, and anecdotal reports from those in Sweden indicate that it’s basically been business as usual there with only minor changes to daily life. This rules out effects from lockdowns strongly affecting the analysis.
Analysis of the whole of Sweden is not ideal, as the virus will not spread evenly throughout the country, and some areas appear to be still significantly affected by COVID-19. For this reason, it will be more helpful to analyse an area which may have passed through the pandemic already and have reached herd immunity.
Stockholm County is the area of Sweden which has been most affected by COVID-191 and the area in which Swedish authorities have informally claimed was going to reach herd immunity by mid-May2. The Folkhälsomyndigheten (Public Health Agency of Sweden) has published “The infection fatality rate of COVID-19 in Stockholm – Technical report”3 which provides detailed information and analysis of COVID-19 in Stockholm County.
Does herd immunity exist?
From the very first moment I heard about the “novel Coronavirus” in Wuhan China, I assumed that herd immunity would eventually stomp it out. It seemed to be spreading too quickly to stop it, and herd immunity seemed to me like the obvious block which would eventually stop it’s spread.
I see many comments online from people who claim that “herd immunity is impossible” or “herd immunity doesn’t work”. These comments seem nonsensical to me. Herd immunity is a standard route to immunity in societies.4 Humankind has relied on this method to wipe out many diseases in the past. Even seasonal influenza is wiped out via herd immunity;5 when it returns, it is usually with a new strain. We now have the influenza vaccine, but before that, natural herd immunity achieved the same effect.
Death vs time plots
My understanding of immunity build up in populations, has always been that when deaths from a disease are plotted over time, there is typically a rise, followed by a fall in deaths. The fall in deaths correlates with herd immunity kicking in. You can see this occurring when countries went into lockdowns, as the number of deaths would rapidly drop. In the case of Stockholm County, they never went into lockdown, and yet the follow plot shows this occurring.
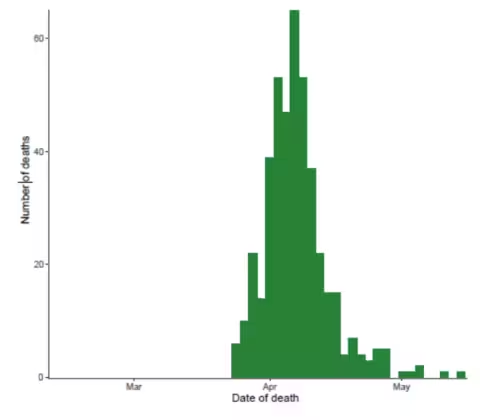
Distribution of date of death in estimation sample
The death vs time plot for Stockholm County matches how I have always understood herd immunity to behave. When I first saw this effect in the raw data, I had falsely assumed that everyone would see this as a very positive thing and no longer fear the number of deaths which may occur from herd immunity. But this effect has been visible in the data coming out of Sweden for months now, and yet people still seem to believe that herd immunity is far off. I do not understand this viewpoint at all.
Anecdotal report from a Swedish MD
On August 4th, Sebastian Rushworth, a Stockholm based MD published a post explaining how COVID-19 hit Stockholm like a storm in mid-March, but after a few months, all the COVID-19 patients had disappeared. His only explanation for the lack of patients is that herd immunity has been achieved there.6
Reinfections
Whenever I mentioned this subject to people in passing, it is common for people to snap back with a comment about herd immunity being impossible because people get reinfected. But if reinfections are a thing, then where are all the reinfected people? There are some reports of reinfections,7 but isn’t this to be expected? Perhaps I am wrong, but I have assumed that if you catch the flu, get over it, then go make out with someone very ill with the same strain of the flu, then there is a good chance you will get sick again. The viral load will be too high for your body to fight off and you will become temporarily sick. That doesn’t mean you weren’t for all intents and purposes “immune”. It just means you weren’t “immune enough” to clear the virus out immediately. There will also be those with poor immune systems who simply struggle to keep it at bay. This is unfortunate for them, but I don’t see this as a reason to fear.
Early on, we only had conjecture and loose on the ground reports from Wuhan China (epicenter of the pandemic) to guide us on how likely reinfections were. Some mass media articles early on indicated that recovered patients had a strong immune response and had become immune.8 Then on June 18th, Chinese researchers published data indicating that only a small drop off in antibody levels were measured in patients with COVID-19.9 A more thorough longer term study by Icelandic researchers was reported on September 1st in which they found no significant drop off in antibody levels even after four months.10
With this data in mind, I feel it is pointless to worry about reinfections being a problem. Perhaps immunity will rapidly drop at some point, but since the immunological response has been strong so far, this seems very unlikely.
Existing and inate immunity
During conversations about herd immunity, I often find that people do not assume that anyone will have natural immunity to COVID-19. I find this very odd, since I thought it was well known that immunity to one strain of influenza can assist with immunity to other strains. Since COVID-19 is a coronavirus, it makes sense to me that some people would likely have cross-immunity to COVID-19 from other coronaviruses or even unrelated viruses.
As far as I am aware, there are no examples of anyone found to have an active antibody response to COVID-19 without having contracted the virus previously. However German researchers have reported that approximately 35% of non-infected people had T-cell responses to COVID-19.11 This does not necessarily mean that 35% of the population is immune, but it may do. There is also the possibility of longer term immunity provided by B cells.12
The human body also has other forms of immunity which are not so easy to test. Presumably for this reason, there is very little data available for these other forms of immunity which may be present.
Herd immunity calculations
The proportion of the community required for herd immunity to be present, can be calculated by the following formula, where R0 is the basic reproduction number13 and pc is the HIT (Herd Immunity Threshold), representing the critical proportion of the population needed to be immune to stop the transmission of disease.14

The R0 for COVID-19 in Wuhan China has been estimated as between 3.8 and 8.9. This gives a required immunity of 74% to 88% for herd immunity.15 This gives us a worst case scenario, as it would be expected that Stockholm would have a lower R0 value than Wuhan did, due to the voluntary social distancing and the distant approach of Swedish people in general.16
In a recent post I wrote about CFR (Case Fatality Rate) vs IFR (Infection Fatality Rate),17 I mentioned a recent COVID-19 IFR literature review published by Professor John Ioannidis of Stanford University, which gave an average IFR value of 0.25%.18, 19 This is the only broad literature review of COVID-19 IFR’s which I have seen, so I’m going to use this for an initial calculation.
Using an IFR of 0.25%, 2384 deaths from COVID-19 in Stockholm County and a total Stockholm County population of of 2.344 million people, we can calculate ~953,000 infected people, which is an infection rate of ~43%. Including the possible 35% immunity from T-cells mentioned earlier, we reach an existing immunity level in Stockholm county of 78%. This is exactly in the ballpark of where a worst case scenario would be based on the R0 value estimated for Wuhan China.
I am making a lot of assumptions here, but my point of doing this calculation is simply to show that herd immunity in Stockholm County does make mathematical sense. It also correlates precisely with what is seen in the death vs time plot shown earlier in this post.
This data of course may not be accurate. The Folkhälsomyndigheten (Public Health Agency of Sweden) technical report that the death vs time plot came from, itself reports an estimated death rate of 0.6%. They also report that based on excess mortality estimates, that the death rate is likely higher by a factor of 1.28, leading to a death rate of ~0.77%. If we plug that number back into the same calculation we come to 13.2% of the population having been infected. Then adding 35% from T-cell immunity we come to 48.2%, which is significantly under the amount required for herd immunity, based on the data from Wuhan. But the data from Wuhan is likely a worst case scenario. Voluntary social distancing, improved overall hygiene and natural distancing in different cultures should be able to drive the level required for herd immunity down considerably.
Conclusion
We don’t have any way to know what the actual IFR or R0 is for Stockholm County. We can only guess. But since the death vs time plot (shown above) indicates that the virus was mostly stamped out of Stockholm County some time ago, I think it is reasonable to suspect that the IFR is likely closer to 0.25% or that the R0 has been kept very low there.
Stockholm may not have reached herd immunity yet, but I would be very surprised if it hasn’t. I would also be very surprised if they have a significant resurgence come winter time. Hopefully I am correct. If I am not, it doesn’t change the point of this article, which was simply to encourage people to look at the data directly rather than regurgitating some dribble they see shared/manipulated by the mass media. Things are rarely as simple as they seem.
Ramifications
If Stockholm County does indeed have herd immunity, then perhaps others do too, or are close behind. This could mean that the policies implemented in countries such as the UK and USA make no sense. If they are also close to herd immunity, then implementing draconian measures to combat the virus doesn’t make sense.
Disclaimer
This was not intended as a scientific paper. I am a scientist (or was), but my background is in synthetic chemistry and drug development; certainly not epidemiology or virology, so I am far from an expert on this subject. I’m just a guy on the internet who is getting frustrated at what he sees online.
Credits
1. Craig Sailor for encouragement and listening to me bleeting on about this subject for months on end.
2. Dr Mauritius Seeger who was the initial source of my frustration, but provided a useful analysis from the polar reverse point of view.
References
1. https://experience.arcgis.com/experience/09f821667ce64bf7be6f9f87457ed9aa
2. Interview with Professor Johan Giesecke – former state epidemiologist of Sweden https://www.youtube.com/watch?v=CfZBzV6kUHw
3. The infection fatality rate of COVID-19 in Stockholm – Technical report – https://www.folkhalsomyndigheten.se/contentassets/53c0dc391be54f5d959ead9131edb771/infection-fatality-rate-covid-19-stockholm-technical-report.pdf
4. Herd Immunity – https://en.wikipedia.org/wiki/Herd_immunity
5. https://www.webmd.com/vaccines/news/20181130/what-herd-immunity-and-how-does-it-protect-us
6. https://sebastianrushworth.com/2020/08/04/how-bad-is-covid-really-a-swedish-doctors-perspective/
7. https://www.theverge.com/2020/8/29/21406019/covid-19-coronavirus-reinfection-immunity-antibodies-vaccine-test
8. Strong immune response to COVID-19 – https://www.nytimes.com/2020/03/25/health/coronavirus-immunity-antibodies.html
9. https://www.nature.com/articles/s41591-020-0965-6
10. https://www.nejm.org/doi/full/10.1056/NEJMoa2026116
11. https://www.nature.com/articles/s41586-020-2598-9
12. B cell immunity https://www.nature.com/articles/s41577-020-00436-4
13. Herd immunity calculations – https://plus.maths.org/content/maths-minute-r0-and-herd-immunity
14. Peer review notes for (6) https://rapidreviewscovid19.mitpress.mit.edu/
pub/k2pkhufi/release/1
15. Wuhan R0 value – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7323562/
16. Swedish lifestyle – https://www.bbc.com/worklife/article/20200328-how-to-self-isolate-what-we-can-learn-from-sweden
17. CFR vs IFR – https://geek.hellyer.kiwi/2020/09/13/covid-19-cfr-vs-ifr/#ref-10
18. Literature review of serology studies – https://www.medrxiv.org/content/10.1101/2020.05.13.20101253v3.full.pdf
19. Peer review notes for (18) https://rapidreviewscovid19.mitpress.mit.edu/
pub/k2pkhufi/release/1
Future post …
We now have sufficient data available to analyse how this panned out. I will write a future post regarding this when I have time. Short version: estimates above were off by a bit, but not hugely so, certainly nothing near the crazy numbers suggested by many on the internet. It seems that the effects of summer arriving were much stronger than I had first estimated. Or it was just randomness. Or it was changes on behaviour in Stockholm. Or it was a more infectious form of the disease. Or it’s a combination of all of those things. But I’ll discuss this in more depth later when I’ve had time to write it and crunch some numbers 🙂
Elisabeth says:
Hi there, I followed your link from a YT comment to read this, and appreciate the work you’ve done here, though confess some of it is dense reading for me! Would love to see an update now that Sweden is in the middle of winter and onlookers seem determined to make a bad example of their approach. Incidentally, I am in NZ, which is also meant to be a different kind of example, but I have some big problems with that, for one the question of whether herd immunity may have already been reached here before lockdown was even considered…
December 28, 2020 at 9:47 am # //
Ryan Hellyer says:
There’s no way NZ ever got anywhere near herd immunity, that’s for sure.
As soon as I can find good up to date data on Stockholm County, I’ll do an update post. I haven’t found any good information on it yet. The Sweden wide data does loosely look it’s supporting the data mentioned here fro Stockholm County though.
January 3, 2021 at 3:12 pm # //
There Is No Pandemic says:
Hi. Find out when the injections were administered and the plot lines may rise and fall in accordance. FYI: [REDACTED]
There was and is no pandemic. It’s a psy-op to terrorize the world into accepting the kill shot. Slow kill, fast kill. Goals: depopulation (the billionaire club has been advocating for it for a long time); and a kick-start for the same gang’s transhumanist project. The injections are loaded with toxic graphene-oxide and self-assembling nano-sized complex micro-tech. Check out Ricardo Delgado on graphene oxide at the site linked above; look for “Ricardo Delgado, La Quinta Columna: Vital Info on the “Human 2.0 Project” — 20,000 Hours of Scientific Research”. And look for “transhumanist”. The World Economic Forum is one of the private billionaire clubs behind the Covid-19 scheme; they’re using it in very detailed precision to achieve the world government they have long been seeking. Look for: “WEF – Covid – 5G – Enhanced Genes – The Great Reset (21 August 2021)” and “UPDATE: WEF – Covid – 5G – Enhanced Genes – The Great Reset (17 July 2022)”. And see: “What Else Are They Hiding in the Vaccines? (by Dr. David Nixon)”. Lots of people have now filmed the stuff in the shots. I’ve also listed a few remedies at that site, for graphene oxide, anyway. And see: [REDACTED]
June 18, 2023 at 7:45 am # //
Ryan Hellyer says:
This is pseudoscience nonsense you are dribbling. I stripped your URLs out; I don’t want to be sharing that sort of thing here.
There are many ways in which the pandemic response can be criticised, but spreading rubbish like this does more harm than good. I think you should stick to sharing science, rather than made up garbage and paranoia.
July 14, 2023 at 1:23 pm # //